Scroll down and use the arrows to view the different case studies from the beginning to the successful end of the patients treatment.
TMJ = Temporomandibular Joint = Jaw Joint
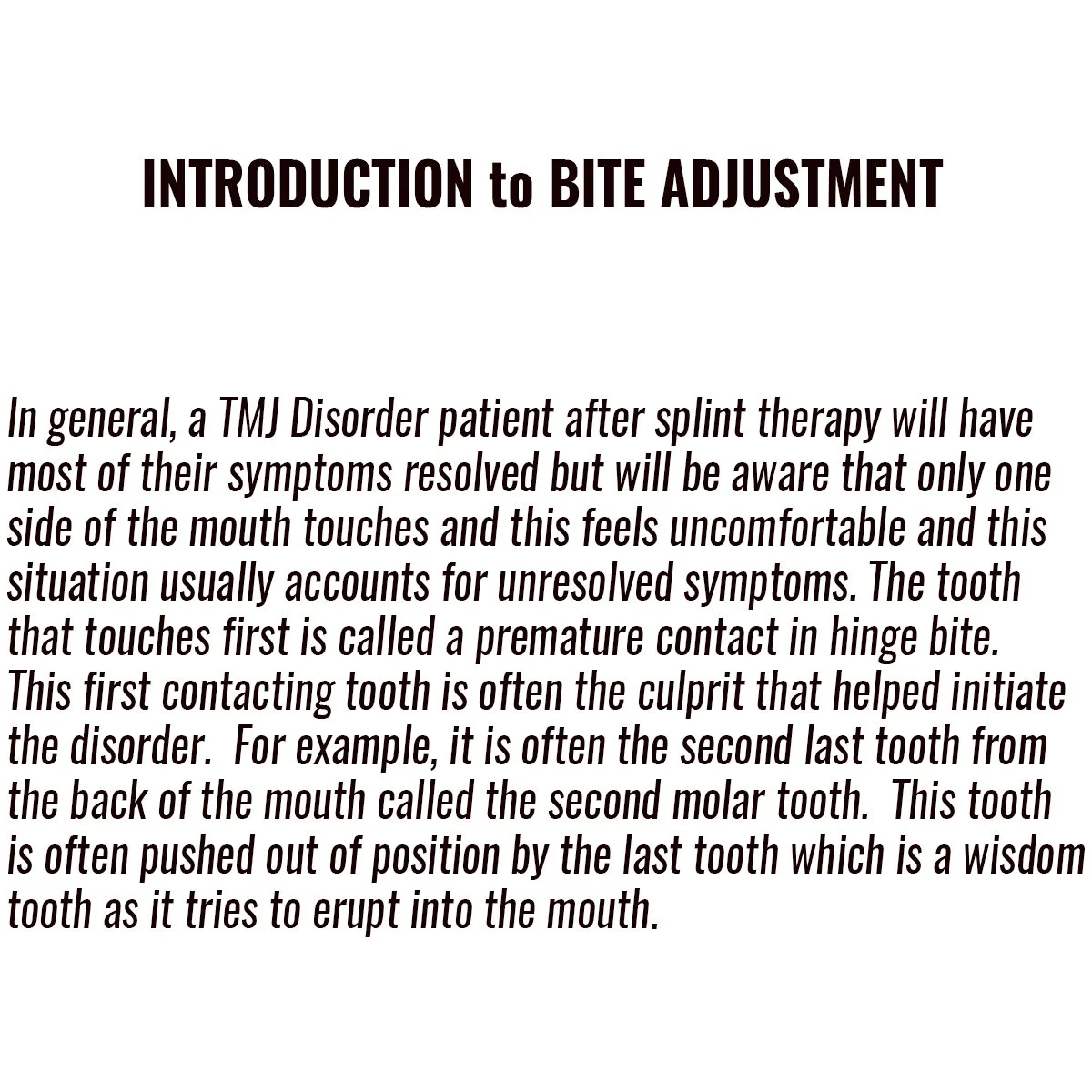
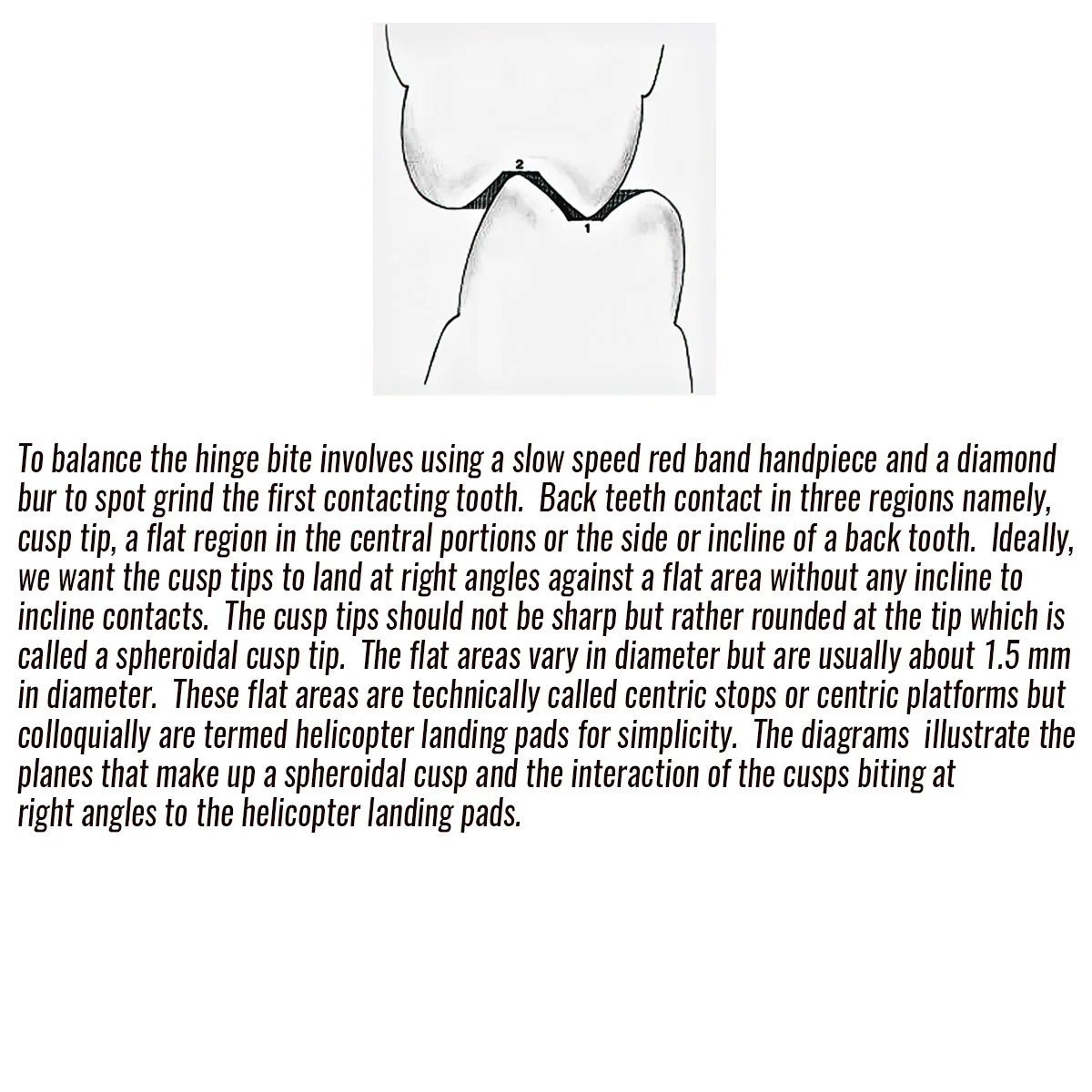
The human jaw joint is a complex joint in the body as it not only hinges in hinge bite but also translates (moves out of the centre of the joint in a straight or curvilinear path) during left, right and forward bites. It relies on the TMJ disc located between the cup and head of the jaw joint which is composed of extremely hard fibrocartilage with different thicknesses. The front of the disc is about 2 mm thick and attaches to the lateral pterygoid muscle. The centre of the disc it is about 1 mm thick and this is where the head (condyle) of the jaw joint rests in hinge bite. The back of the disc is about 3 mm thick and it attaches to the posterior elastic ligament. This elastic ligament is responsible for relocating the disc back into the centre of the jaw joint following translation in left, right and forward bites. The position of the teeth is important in maintaining the head and disc in the centre of the jaw joint. If in hinge bite for example only the last molar tooth makes contact first (called a premature contact in the diagram) then this will throw out the lower jaw off centre and the position of the disc. When the disc is off centre it is called a displaced disc.


Full Occlusal Therapy for a Temporomandibular Disorder (TMD)
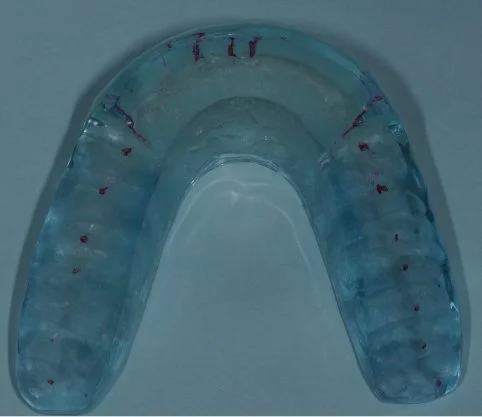
A TMJ Disorder patient requires conservative management with “Full Occlusal Therapy” in 3 stages along with concurrent Full Counselling (refer to journal papers 19 and 20). In other words, we need to get the disc back into the centre of the joint where it belongs starting with Full Counselling and then a Fully Protective Occlusal Splint (Stage 1). This splint is made of acrylic resin (used for dentures) and can be made in clear resin but is usually coloured blue or pink to hide any future discolouration (as in the photos below). The splint usually fits the upper teeth and only one is required.
This diagram illustrates a disc that is displaced out of the socket and the elastic ligament is very stretched because the first contacting molar tooth in hinge bite has been avoided by the lower jaw. The lower jaw has moved forward and to one side to escape this erroneously positioned tooth. The result as displayed in this diagram shows all the teeth meshing to be able to now eat. However, the head is no longer positioned in the centre of the jaw joint and the disc is displaced. The patient now has a clicking disc and the beginning of a TMJ Disorder which is abbreviated TMD.
Full Occlusal Therapy is sequential:
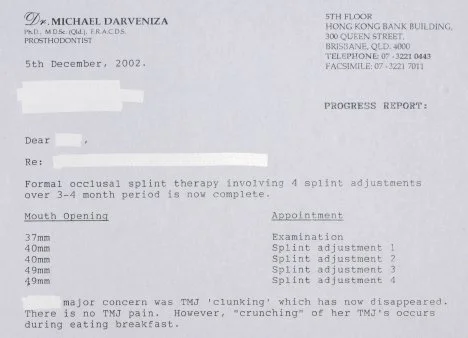
Stage 1 - Fully Protective Occlusal Splint - 4 SA’s over a 3 month period
Stage 2 - Occlusal equilibration - major OA then 2 fine tune adjustments over a 7 month period
Stage 3 - Bio-Designing Molar Guidance or Anterior Guidance or Orthodontics
with concurrent Full Counselling
Not all TMJ patients require all 3 stages as it depends on how unprotected their 4 bites of hinge, left, right and forward are after splint therapy.
INTRODUCTION TO OCCLUSAL SPLINTS
-
![]()
-
![]()
COLOURED ACRYLIC RESIN SPLINTS FOR UPPER TEETH BEFORE FITTING- 2 different patient cases
-
![]()
MEDIUM THICKNESS LIGHT PINK UPPER SPLINT 13 YEAR OLD GIRL TMJ DISORDER
-
![]()
-
![]()
-
![]()
-
![]()



Stage 1 of Full Occlusal Therapy is Formal Fully Protective Occlusal Splint Therapy with case study
-
![]()
THIS PATIENT HAS A SERIOUS GRINDING OR BRUXING HABIT THAT WAS INTERCEPTED BEFORE HE DESTROYED ALL HIS TEETH. THIS PHOTO SHOWS A LEFT UNPROTECTED BITE WITH COW LIKE JAW MOVEMENT WHICH NOT ONLY ALLOWED THE WEAR TO ACCELERATE BUT ALSO DAMAGED HIS TMJ JAW JOINTS WITH PAIN CLUNKING AND RESTRICTED MOUTH OPENING.
-
![]()
-
![]()
-
![]()
-
![]()
-
![]()
RED MARKINGS INDICATING BALANCED HINGE BITE AND LONG GUIDING AND CENTRING PATHS FOR FORWARD, RIGHTAND LEFT EXTREME JAW MOVEMENTS
-
![]()
PROTECTIVE HINGE BITE AND THICK SPLINT TO RELAX GRINDING MUSCLES
-
![]()
PROTECTIVE FORWARD BITE
-
![]()
PROTECTIVE RIGHT BITE
-
![]()
PROTECTIVE LEFT BITE
-
![]()
THIS PATIENT HAD MANY SYMPTOMS RESOLVED FROM SPLINT THERAPY BUT WHEN EATING THE JAW JOINTS CRUNCHED BECAUSE IN HINGE BITE ONLY THE LEFT SIDE OF THE MOUTH WAS BITING. TO RECTIFY THIS, THE PATIENT MOVED ON TO STAGE 2 INVOLVING BITE ADJUSTMENT WHICH INVOLVED SPOT GRINDING THE LEFT SIDE TEETH TO SOLVE THE CHEWING/JAW JOINT CRUNCHING PROBLEM.





Stage 2 of Full Occlusal Therapy
Occlusal Equilibration = Occlusal Adjustment = Bite Adjustment
-
![]()
-
![]()
-
![]()
-
![]()
Full mouth reconstruction in 1990 with crowns in protective hinge bite with bilateral tooth contacts
-
![]()
-
![]()
Full mouth occlusal reconstruction in 1990 with crowns illustrating right protective bite
-
![]()
-
![]()
-
![]()
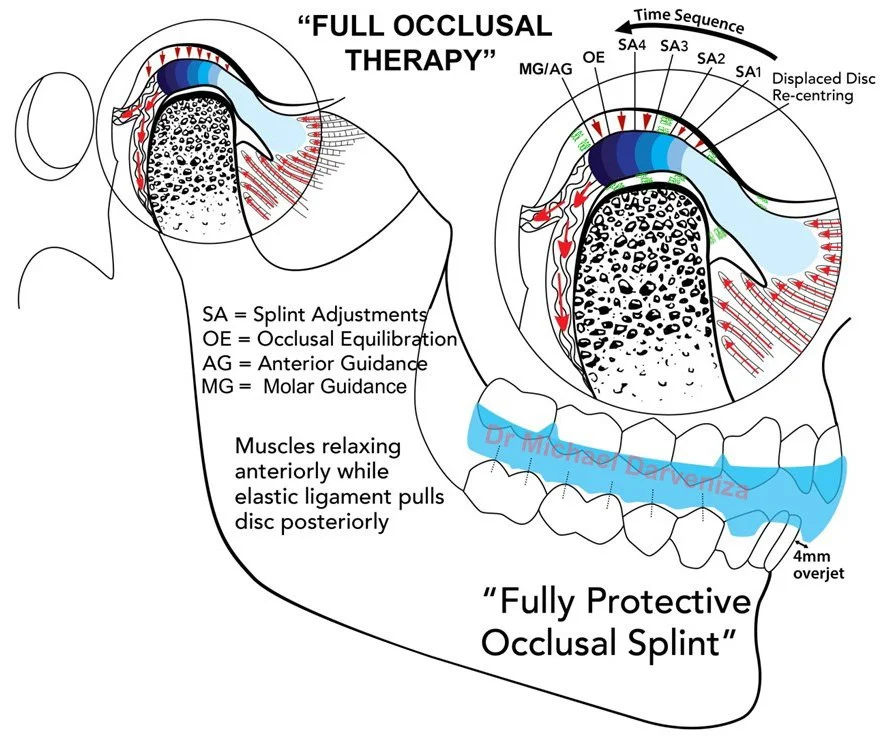
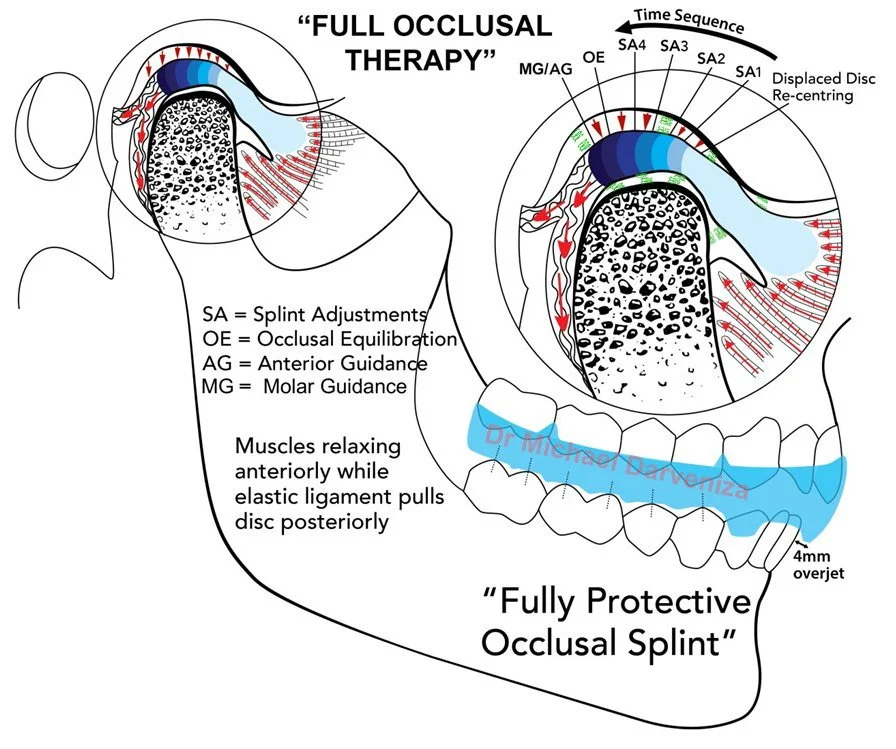
THE ABOVE DIAGRAM ILLUSTRATES THE SEQUENTIAL CHANGES IN THE TMJ DISCS AND MUSCLE LENGTHS DURING FULL OCCLUSAL THERAPY.

Case Study
-
![]()
-
![]()
-
![]()
-
![]()
-
![]()
BEFORE - ILLUSTRATES THE TOP LEFT BACK TEETH WITH RED MARKINGS FROM ARTICULATING PAPER INDICATING WEDGING BITE INTERFERENCES ON THE MOLARS.
-
![]()
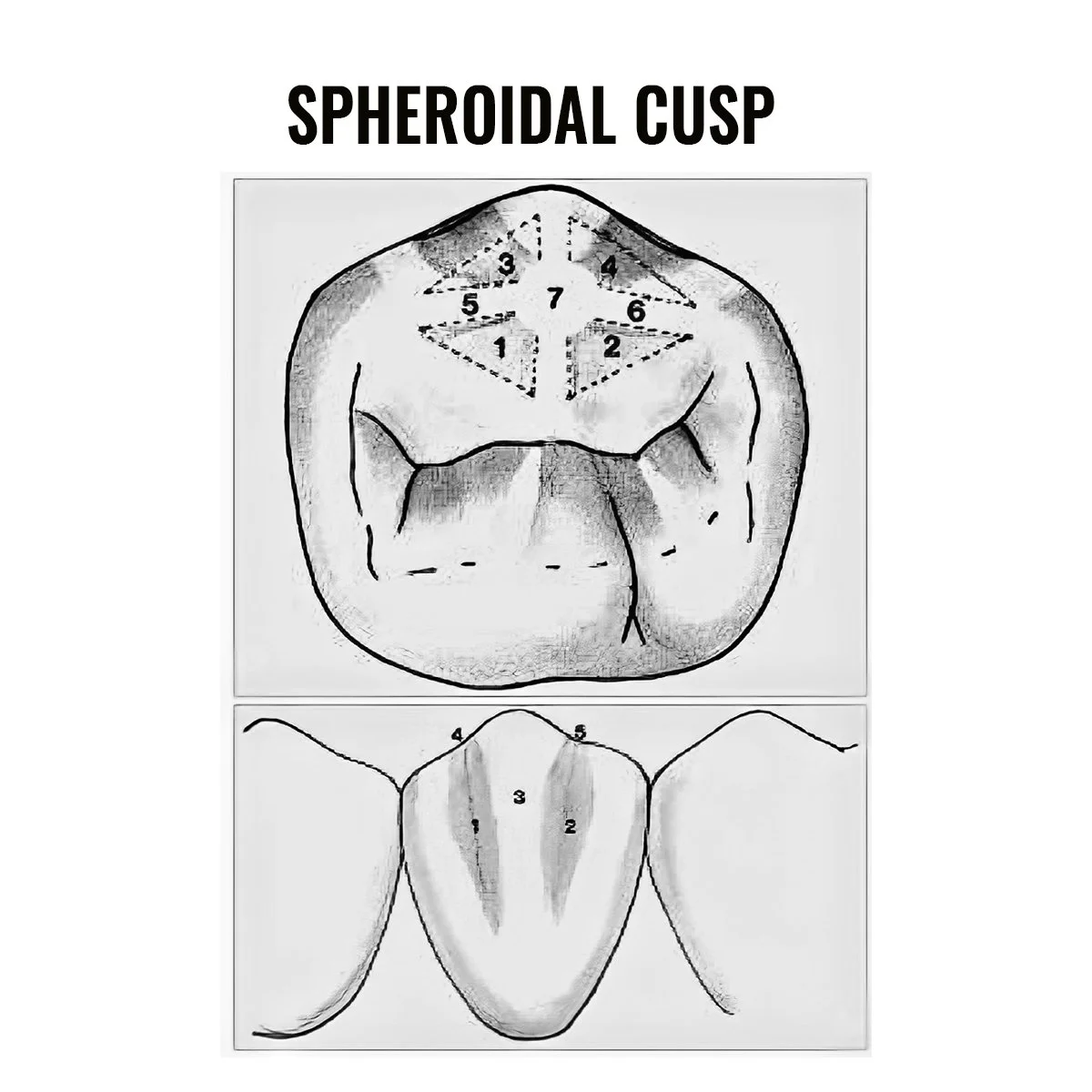
AFTER- ILLUSTRATES AN IDEAL BITING RELATIONSHIP WITH CONTACTING CUSP TIPS AND FLAT ’HELICOPTER’ BITING PLATFORMS WITH EQUAL INTENSITY OF RED MARKS. THE OTHER TEETH IN THE MOUTH WERE SIMULTANEOUSLY ADJUSTED TO FINALISE A BILATERAL PROTECTIVE HINGE BITE.
-
![]()


Stage 3 of Full Occlusal Therapy – Orthodontics or Anterior Guidance or Molar Guidance
After Bite Adjustment the key teeth that guide the lower jaw left, right and forward are often mal-positioned or worn away and need to be repositioned or built up. These mal-positioned/worn teeth allow the lower jaw to skid around with cow like jaw movements which continue to stretch jaw joints resulting in TMJ and facial clenching muscle pains. These teeth need to be bio-designed to form optimal tooth shapes to create protective left, right and forward bites. The conservative first choice is to orthodontically reposition mal-positioned teeth.
Many TMJ pain patients are not interested in doing years of orthodontic treatment and would prefer an instant Prosthodontic solution. This generally involves building up teeth with composite resin overlays or crowns.
CASE STUDY 1
PROTECTIVE CROWNS FOR BIO-DESIGNING LEFT AND RIGHT JAW MOVEMENTS
-
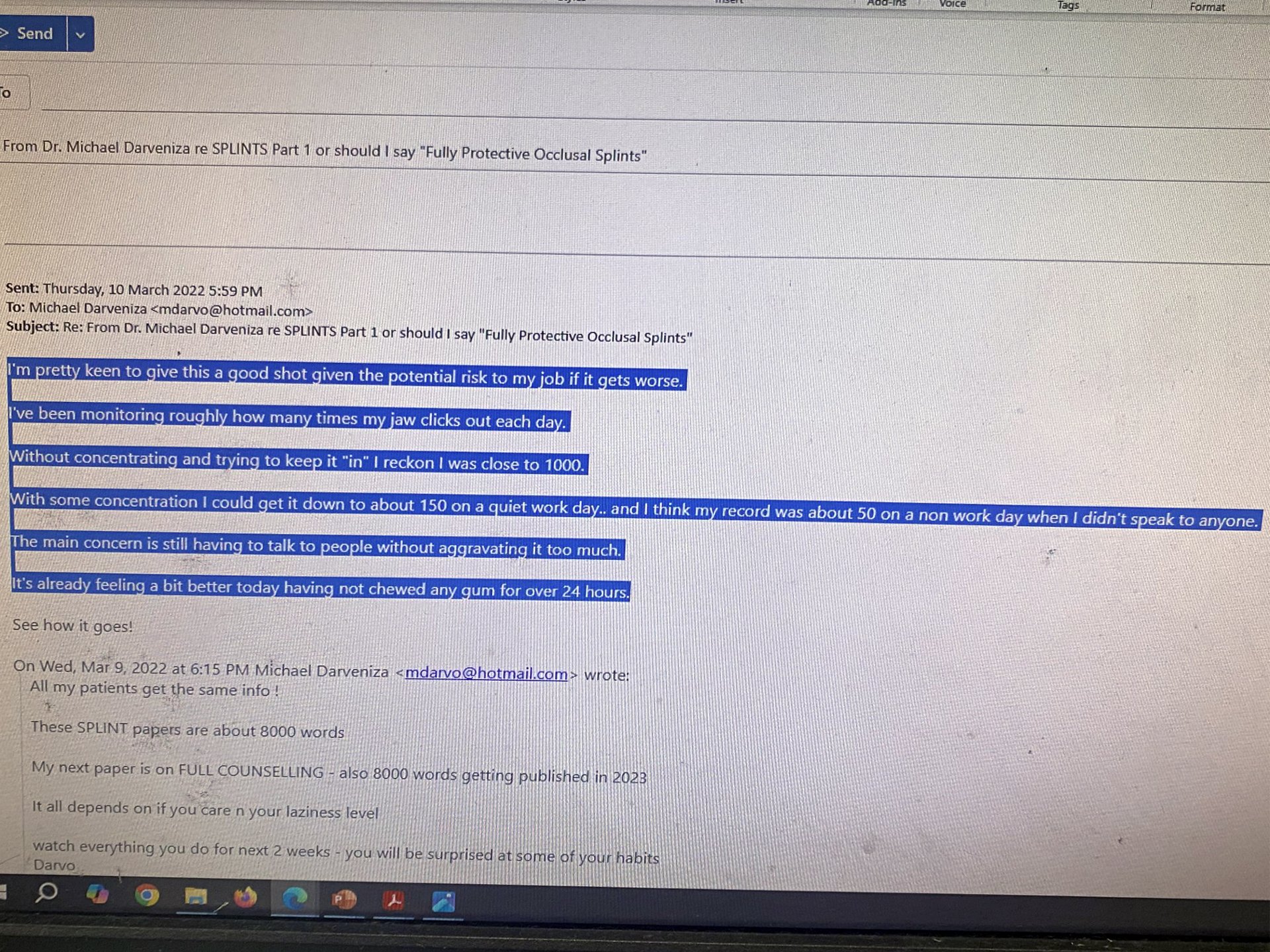
![Text discussing dental treatment for TMJ issues and canine teeth adjustment.]()
-
![Close-up of human teeth showing bite alignment and dental health]()
The lower left canine is impacted and in an unprotected left jaw movement involving an extreme left movement called crossover. This crossover position shows wedging of the adjacent lower left lateral incisor between the two top teeth namely the left lateral incisor and left canine. This extreme crossover allowed the left jaw joint to dislocate quite often.
-
![Close-up of human teeth showing overbite, misalignment, and yellowish tint.]()
The lower right canine is unnaturally positioned and impacted against the adjacent lower right lateral incisor and being very short in stature resulting in a right unprotected cow like jaw movement. This unprotected right jaw movement allowed the contralateral left jaw joint to dislocate quite often.
-
![Dental plaster model of human teeth]()
A plaster model of the prepared lower canine teeth ready for fabrication of Zirconia/porcelain crowns.
-
![Dental plaster model with a ceramic tooth]()
The completed crowns in the mouth while the jaw was in protective right and left jaw movements. Please note the pseudo ‘microcracks’ built into the body of the crown using ceramic artistry with caramel porcelain to copy and match the adjacent microcracked natural teeth.
-
![Dental mold with prosthetic tooth]()
The colour of these teeth on these models is not indicative of what it will look like in the mouth.
-
![Close-up of a person's teeth and gums showing dental alignment and condition.]()
The completed crowns in the mouth while the jaw was in protective right and left jaw movements. Please note the pseudo ‘microcracks’ built into the body of the crown using ceramic artistry with caramel porcelain to copy and match the adjacent microcracked natural teeth.
-
![Close-up of human teeth and gums showing upper and lower incisors and canines.]()
The patient has been using the crowns for about 2 years and no longer has dislocation and locking of the lower jaw after Full Occlusal Therapy (Paper 14-Darveniza M. Full occlusal protection – theory and practice of occlusal therapy. Australian Dental Journal 2001;46(2):70)







CASE STUDY 2
PROTECTIVE COMPOSITE RESIN OVERLAYS FOR BIO-DESIGNING LEFT AND RIGHT JAW MOVEMENTS
-
![]()
-
![]()
THIS PHOTO OF A 20 YEAR OLD PATIENT SHOWS PREMATURE WEAR OF THE LOWER RIGHT CANINE TOOTH FROM EXCESSIVE NOCTURNAL GRINDING OR BRUXISM.
-
![]()
THE LEFT SIDE PHOTO SHOWS THE PREPARED TOOTH WITH CLEAR STRIPS AND WOODEN WEDGES PLACED TO HELP FORM A NEW CUSP USING A COMPOSITE RESIN OVERLAYING TECHNIQUE. THE RIGHT SIDE PHOTO SHOWS THE COMPLETED RIGHT PROTECTIVE BITE WITH THE CANINES ENGAGING TO CREATE VERTICO-LATERAL HUMAN LOWER JAW MOVEMENT.
-
![]()
THE LEFT PHOTO SHOWS THAT THE LOWER LEFT CANINE TOOTH IS POSITIONED INCORRECTLY AND TOO FAR BACK IN THE MOUTH, IN HINGE BITE. THE RIGHT PHOTO SHOWS WHEN THE LOWER JAW MOVES TO THE LEFT THE CANINES DO NOT ENGAGE AND THE JAW MOVED BACKWARDS TOWARDS THE EAR RESULTING IN LEFT TMJ PAIN AND TINNITUS.
-
![]()
THE LEFT PHOTO SHOWS THAT THE LOWER JAW WHEN MOVING TO THE LEFT AND FORWARD ALLOWING A NASTY WEDGING CONTACT TO FORM BETWEEN THE TOP LEFT CANINE AND THE LOWER LEFT NO. 2 LATERAL INCISOR TOOTH WHICH CREATED FACIAL PAINS. THE RIGHT PHOTO SHOWS THE PREPARED TOP LEFT CANINE TOOTH PRIOR TO OVERLAYING WITH COMPOSITE RESIN.
-
![]()
THE LEFT PHOTO SHOWS THE COMPLETED COMPOSITE OVERLAY ON THE TOP LEFT CANINE TOOTH BUT STILL WITH A WEDGING CONTACT ON THE LOWER TEETH. THE RIGHT PHOTO SHOWS THE PREPARED LOWER LEFT LATERAL INCISOR AND CANINE TOOTH PRIOR TO OVERLAYING.
-
![]()
THE LEFT PHOTO ILLUSTRATES THE COMPLETED PROTECTIVE LEFT JAW MOVEMENT. THE RIGHT PHOTO ILLUSTRATES THE COMPLETED CUSPS OF THE LOWER CANINES. THESE BIO-DESIGNED LEFT AND RIGHT BITES STABILISED THE LOWER JAW AND THE PATIENT’S TINNITUS, TMJ AND FACIAL MUSCLE PAINS CESSATED.






Mission Statement
“As a dedicated experienced clinician my goal is to listen intently to patient’s concerns, issues and their dental requirements. My examination involves a tactile appreciation of their symptoms and a visual inspection of their immediate dental concerns. Dental problems that confront me I find a challenge to solve. My approach involves addressing patient’s emotional requirements followed by my knowledge in engineering, design, material science and aesthetic dental science to problem solve in a holistic manner. The fundamental requirements of conservative management are mandatory to conserve tooth structure, wherever possible, and to find the easiest and least expensive solution while not compromising longevity of dental restorations and prostheses. In every instance creating a dental environment to minimise pain during dental procedures is paramount. I look forward to helping you with your dental treatment to get the very best results performed in a light and cheerful manner.”
Yours sincerely,
Michael Darveniza


SURF ABU DHABI
March 2025